A prolactinoma is the most common type of pituitary adenoma - a benign tumor in the pituitary gland that overproduces the hormone prolactin. While many people have small pituitary tumors without ever knowing it, prolactinomas are different. They cause real, noticeable changes in your body because of the hormone chaos they create. In women, this often means missed periods, breast milk production even when not pregnant, and trouble getting pregnant. In men, it can lead to low libido, erectile dysfunction, and even breast enlargement. These aren’t rare side effects - they happen in over 90% of women and 80% of men with untreated prolactinomas.
What Exactly Is a Pituitary Adenoma?
The pituitary gland is a tiny pea-sized organ at the base of your brain. It’s often called the "master gland" because it controls other hormone-producing glands like the thyroid, adrenal glands, and ovaries or testes. When a tumor grows here - even if it’s not cancerous - it can mess with hormone signals in two ways: by making too much of one hormone, or by pressing on the gland and stopping it from making others.
About 1 in 10 people have some kind of pituitary growth, but only a small fraction cause symptoms. Prolactinomas make up 40% to 60% of all hormone-producing pituitary tumors. They’re classified by size: microadenomas are under 1 cm (about the size of a pea), and macroadenomas are larger than 1 cm. Macroadenomas are more likely to cause problems like vision loss because they can press on the optic nerve.
How Do Prolactinomas Disrupt Hormones?
Prolactin’s normal job is to help with breast milk production after childbirth. But when a tumor floods your system with extra prolactin, it throws off the whole hormone balance. High prolactin shuts down the signals that tell your ovaries or testes to make estrogen and testosterone. That’s why women stop menstruating and men lose sexual drive. It also lowers bone density over time, increasing fracture risk.
Doctors look for prolactin levels above 150 ng/mL - that’s 95% specific for a prolactinoma. Levels over 200 ng/mL almost always mean a macroadenoma. A simple blood test can catch this, but it’s not foolproof. Stress, pregnancy, kidney failure, and even certain medications can raise prolactin too. That’s why an MRI of the pituitary is always needed to confirm.
How Is It Diagnosed?
Diagnosis starts with a blood test for prolactin. If it’s high, the next step is a high-resolution MRI of the pituitary with 3mm slices. This shows the tumor’s size and whether it’s pushing into nearby structures. For tumors larger than 1 cm, doctors also check your vision with a visual field test. You might be asked to identify flashing lights in your peripheral vision - if you miss them, the tumor may be pressing on your optic nerves.
It’s important to rule out other causes of high prolactin. If you’re on antidepressants, antipsychotics, or even some stomach meds, those could be the culprit. Pregnancy and breastfeeding are obvious ones. But if none of those fit, and your MRI shows a tumor, it’s almost certainly a prolactinoma.

Treatment: Medication Is First
For almost all prolactinomas, the first treatment is a dopamine agonist - a drug that tricks the brain into thinking there’s enough prolactin already. The two main ones are cabergoline and bromocriptine. Cabergoline is now the go-to choice. It works better, has fewer side effects, and only needs to be taken once or twice a week. Bromocriptine requires daily doses and often causes nausea, dizziness, or low blood pressure.
Studies show cabergoline normalizes prolactin levels in 80-90% of microadenomas and about 70% of macroadenomas within three months. Tumor shrinkage happens in 85% of cases. One case from Mayo Clinic followed a woman with a 2.4 cm tumor and a prolactin level of 5,200 ng/mL. After six months on cabergoline, her levels dropped to 18 ng/mL and the tumor shrank by 70%.
Most people start with 0.25 mg twice a week. The dose is slowly increased every few weeks based on blood tests. Side effects like nausea or lightheadedness usually fade after a few weeks. If they don’t, lowering the dose temporarily helps. A small number of people (about 2-7%) on long-term, high-dose cabergoline (over 2 mg per week) may develop heart valve issues. That’s why doctors recommend an echocardiogram after one year of treatment.
When Is Surgery Needed?
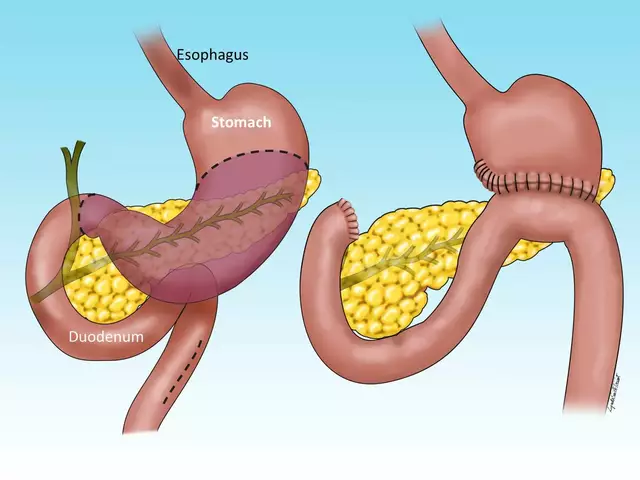
Surgery isn’t the first option - but it’s life-changing for some. Transsphenoidal surgery means removing the tumor through the nose. It’s minimally invasive, leaves no facial scars, and most patients go home in 3-5 days. Success rates are high for small tumors: 85-90% of microadenomas are fully removed. But for macroadenomas, especially those that have grown into the cavernous sinus (where major blood vessels sit), success drops to 35-50%.
Doctors usually recommend surgery if:
- Medication doesn’t work or causes unbearable side effects
- The tumor is pressing on the optic nerve and threatening vision
- The patient wants to get pregnant and can’t tolerate long-term drugs
Still, surgery has risks. About 5-10% of patients develop diabetes insipidus - a condition where the body can’t hold water - and need daily desmopressin. CSF leaks (fluid from the brain) happen in 2-5% of cases. And in about 1-2% of cases, sudden bleeding into the tumor (pituitary apoplexy) requires emergency surgery.
Radiation Therapy: A Last Resort
Radiation is rarely used today, mostly for tumors that won’t shrink with meds or surgery. Options include Gamma Knife radiosurgery (one high-dose session), conventional radiation (given daily over weeks), or proton therapy.
Gamma Knife controls tumor growth in 95% of cases after five years and causes less damage to surrounding tissue than older radiation methods. But it doesn’t fix hormone problems fast. It can take 2-5 years for prolactin levels to drop. And about 30-50% of patients end up with low levels of other pituitary hormones (hypopituitarism) within 10 years - meaning they’ll need lifelong hormone replacement.
Most patients who get radiation say they still felt symptoms for over a year. But by year three, 85% saw improvement. It’s slow, but it works when nothing else does.
Life After Diagnosis
Many people worry about lifelong medication. But here’s the truth: over 70% of people with prolactinomas need to stay on dopamine agonists indefinitely. Stopping the drug, even for a few days, can cause prolactin to spike again within 72 hours. That’s why consistency matters.
Monitoring is key. Blood tests every three months at first, then once a year if things are stable. MRIs every one to two years. Vision checks if you had a large tumor. And if you’re on cabergoline long-term, get your heart checked every two years.
Women who want to get pregnant can often stop medication under supervision. Prolactin levels usually drop naturally during pregnancy, and the tumor rarely grows. But close monitoring is still needed.
For men, restoring testosterone levels often brings back energy, mood, and sex drive. Bone density improves with treatment, reducing fracture risk.
What’s Coming Next?
New drugs are on the horizon. A medication called paltusotine, already approved for acromegaly, is being tested for prolactinomas. It might offer better control with fewer side effects. Researchers are also looking at gene therapy - using CRISPR to fix mutations linked to tumor growth. AI is helping surgeons plan more precise removals by mapping tumor boundaries in 3D.
But for now, the best approach remains simple: catch it early, treat with cabergoline, and stick with it. Most people go on to live full, healthy lives - with normal hormone levels, fertility, and no major complications.
Can prolactinomas become cancerous?
No, prolactinomas are almost always benign. They don’t spread to other parts of the body like cancer. But even though they’re not cancerous, they can still cause serious problems by pressing on the brain or disrupting hormones. That’s why treatment is important.
Is cabergoline safe for long-term use?
Yes, for most people. Cabergoline has been used safely for over 30 years. The main concern is heart valve changes at very high doses (over 2 mg per week). That’s why doctors limit the dose and recommend an echocardiogram after one year. For patients on lower doses, the risk is extremely low. The benefits of normalizing hormones and shrinking the tumor far outweigh the risks for nearly everyone.
Can I get pregnant if I have a prolactinoma?
Absolutely. Many women with prolactinomas conceive after starting cabergoline, which restores ovulation. Some women stop the medication under their doctor’s guidance once pregnant, as prolactin levels naturally rise during pregnancy. The tumor rarely grows during pregnancy, but regular monitoring with an endocrinologist is essential.
Why do some people need surgery instead of medicine?
Surgery is considered when medication doesn’t work, causes intolerable side effects, or when the tumor is so large it’s threatening vision or other brain structures. In these cases, removing the tumor quickly is more urgent than waiting for drugs to shrink it. Surgery is also chosen by patients who want to avoid lifelong medication.
Do I need to take medication forever?
About 70% of people need to stay on dopamine agonists long-term. Even if the tumor shrinks and prolactin normalizes, stopping the drug often causes it to come back. Some patients with small tumors may be able to stop after several years of stable results - but only under close medical supervision. Never stop on your own.




Luke Trouten
February 13, 2026 AT 01:59Prolactinomas are a fascinating example of how a tiny structure can derail an entire endocrine system. The pituitary isn't just a gland-it's the conductor of the hormonal orchestra, and when one section goes rogue, the whole symphony falls apart. What's remarkable is how precisely dopamine agonists restore balance. It's not just suppression-it's negotiation. The body still has its signals; we're just giving it the right feedback loop. This is neuroendocrinology at its most elegant.
And yet, we treat it like a simple hormone replacement problem. It's deeper than that. It's about identity, fertility, and the invisible ways our biology shapes our sense of self. A man losing libido isn't just 'low testosterone'-he's losing a part of how he experiences connection. A woman missing periods isn't just 'anovulation'-she's grieving a future she thought was guaranteed. Medicine fixes the tumor. But healing takes more.
Kristin Jarecki
February 13, 2026 AT 21:50Thank you for this comprehensive overview. The clinical precision in detailing diagnostic thresholds, treatment protocols, and monitoring guidelines is invaluable. I would like to emphasize the importance of distinguishing between pharmacologically induced hyperprolactinemia and true prolactinomas, as misdiagnosis can lead to unnecessary imaging or inappropriate treatment. Additionally, the long-term cardiac monitoring recommendation for patients on cabergoline above 2 mg/week is clinically sound and aligns with current endocrine society guidelines. Consistent follow-up with an endocrinologist remains paramount, particularly in cases of macroadenomas or pregnancy planning.
Jonathan Noe
February 15, 2026 AT 01:33Bro, I had a prolactinoma. 5,200 ng/mL. 2.4 cm. They said I’d be on meds forever. Six months on cabergoline, tumor’s gone, prolactin’s normal. I’m not joking-my libido came back like I was 19 again. And my wife? She got pregnant on the third try after I stopped the meds. No surgery. No radiation. Just one pill twice a week. People think this is some rare disease? Nah. It’s underdiagnosed. I’m telling you, if you’re tired, low sex drive, weird milk leakage? Get your prolactin checked. Don’t wait. I waited two years. Don’t be me.
Jim Johnson
February 15, 2026 AT 04:25Man, I wish I knew this 10 years ago. I thought I was just 'getting old'-low energy, no interest in sex, mood swings. Doc said 'stress' and gave me SSRIs. Then I started leaking milk. Not from a baby. From me. 😳 I Googled it. Came here. Found out I had a macroadenoma. Cabergoline fixed everything. I’m 38 now, married, had a kid. Still on meds. But I’m alive. And I’m not depressed. Just… normal. If you’re reading this and you’re like I was-don’t ignore it. Get tested. It’s not embarrassing. It’s biology.
Autumn Frankart
February 15, 2026 AT 12:16They say it's a tumor. But what if it's a signal? What if the body is screaming because the system is broken? Who controls the pituitary? Who controls the doctors who control the meds? Cabergoline is a dopamine mimic-but dopamine is the neurotransmitter of control. Are we really fixing the tumor… or are we silencing the body's rebellion against a system that’s been poisoning us with processed food, EMF, and pharmaceutical dependency? The FDA approved this drug in 1998. Coincidence? Or part of the agenda? I’ve seen the data. The heart valve risks? They’re buried. They don’t want you to know. You’re being managed. Not healed.
Skilken Awe
February 17, 2026 AT 02:26Oh wow, another 'I had a prolactinoma and now I'm fine' testimonial. Let me guess-you got lucky with a microadenoma and stopped after 6 months. Meanwhile, the real patients? The ones with 10 cm tumors crushing their optic nerves? They’re the ones who need surgery. But no, let’s just pat ourselves on the back and say 'meds work' while ignoring the 15% of cases where cabergoline fails. And don’t even get me started on the fact that 70% need lifelong treatment. That’s not a cure. That’s a life sentence. And you’re celebrating it like it’s a win? Pathetic.
Steve DESTIVELLE
February 18, 2026 AT 05:42Life is a series of imbalances and the pituitary is the silent witness to all of them. The tumor is not the disease it is the symptom of a deeper dissonance between the self and the environment. Modern medicine seeks to remove the symptom without addressing the cause. We live in a world of artificial light and artificial rhythms and our glands are confused. The dopamine agonist is a bandage on a wound that is bleeding from within. The real cure is not in a pill but in the return to natural cycles. To darkness. To silence. To the moon. To the earth. To the body that once knew how to heal itself before the lab coats came with their vials and their algorithms.
And yet I understand the need for intervention. For survival. For fertility. For the right to feel whole. So I do not reject the science. I transcend it. The pill is a bridge. Not the destination.
Ernie Simsek
February 18, 2026 AT 10:59I just got my prolactin levels back today. 18. Normal. 🤯 I’ve been on cabergoline for 2 years. Still taking it. Still alive. Still married. Still got my sex drive back. My wife says I’m 'less moody'. I say I’m 'not a zombie anymore'. 🧠💊 You’re not broken. You’re just out of balance. Get tested. Don’t be a hero. Just take the pill. 💪❤️